
Efficacy of 12-lead vs 15-lead ECG on diagnostic delays and clinical outcomes in isolated posterior STEMI: A Case in Point
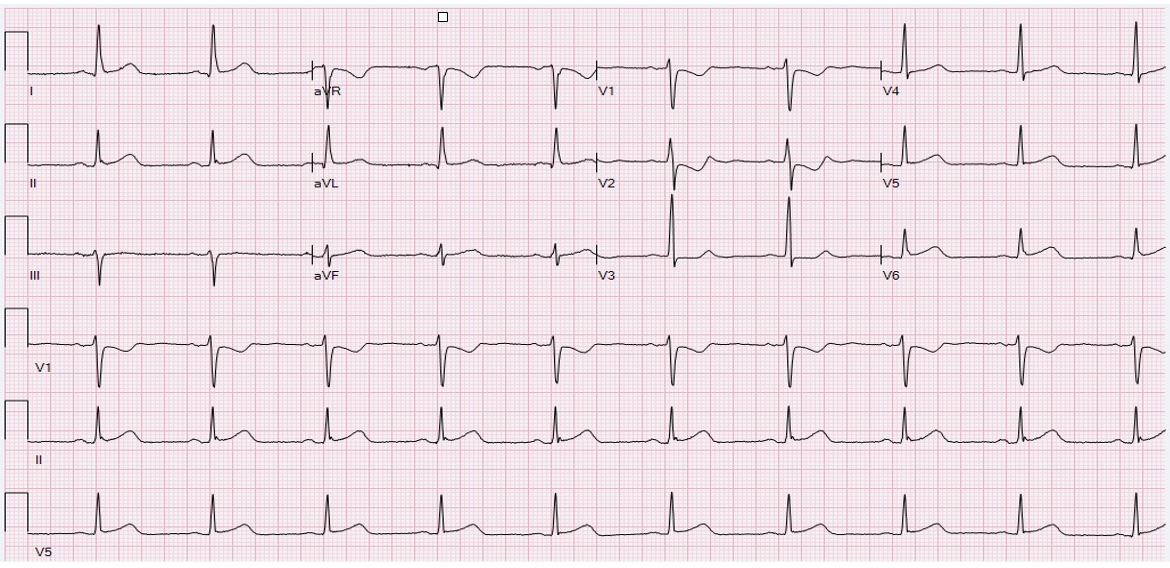
The following series of ECG’s from a posterior STEMI that presented to the ER at 5:30 AM, illustrates the importance of early 15-lead ECG. The initial 12-lead showed profound ST-depression (STD) in V1-V2, and minimal STD in V3 (below).
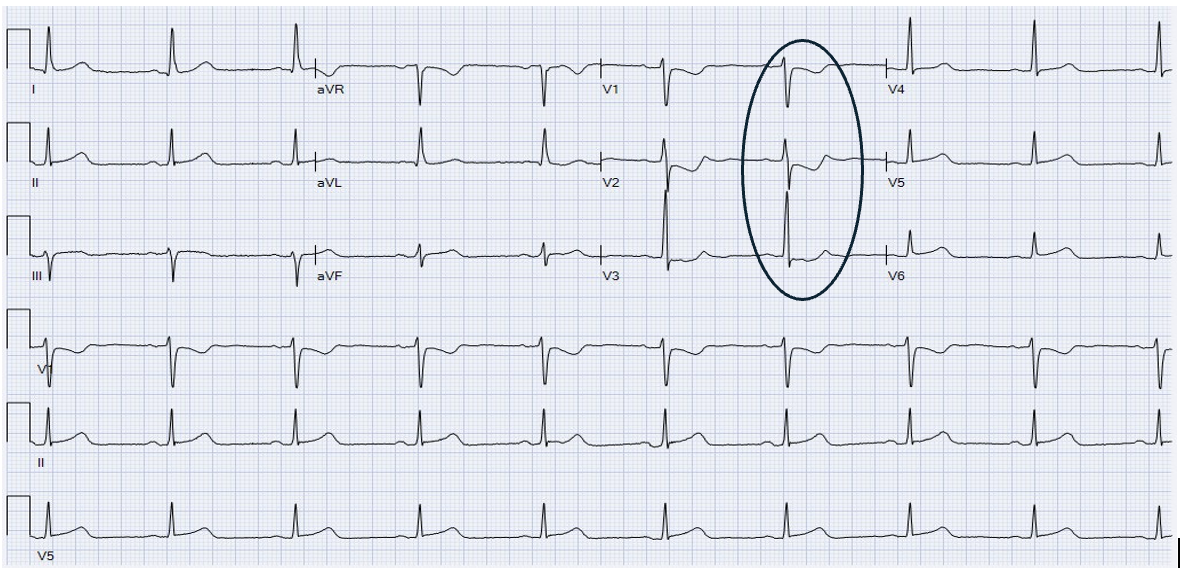
A repeat 12 lead at 6:00 AM showed worse STD:
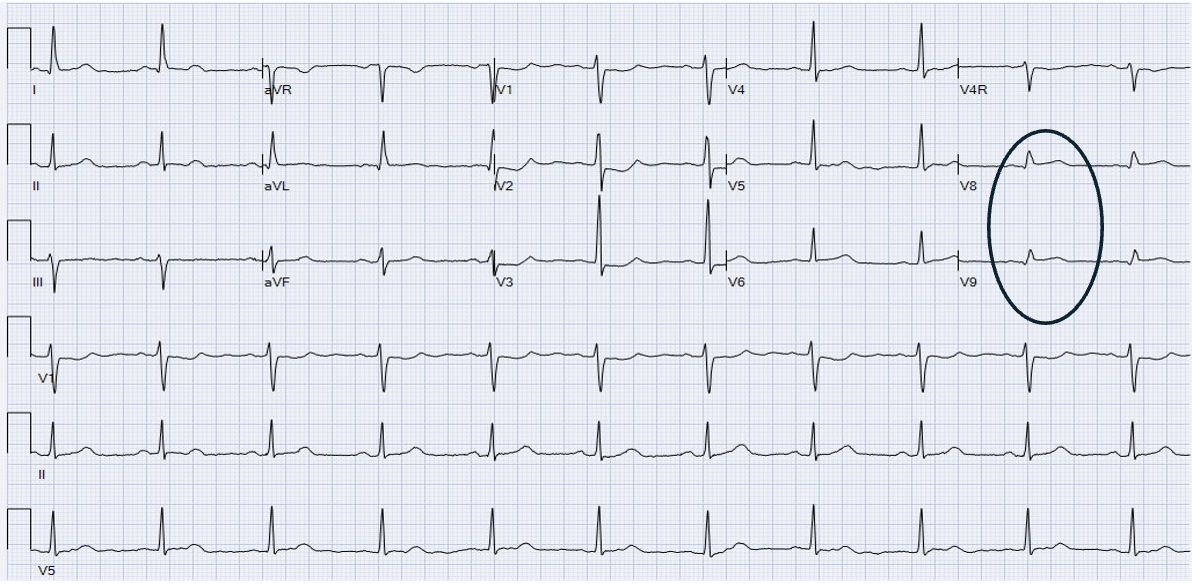
A posterior STEMI wasn’t recognized until a 15-lead ECG was finally performed at 9:30 AM, causing a diagnostic delay of 4 hours. ST-elevation (STE) in V8-V9 is evident.
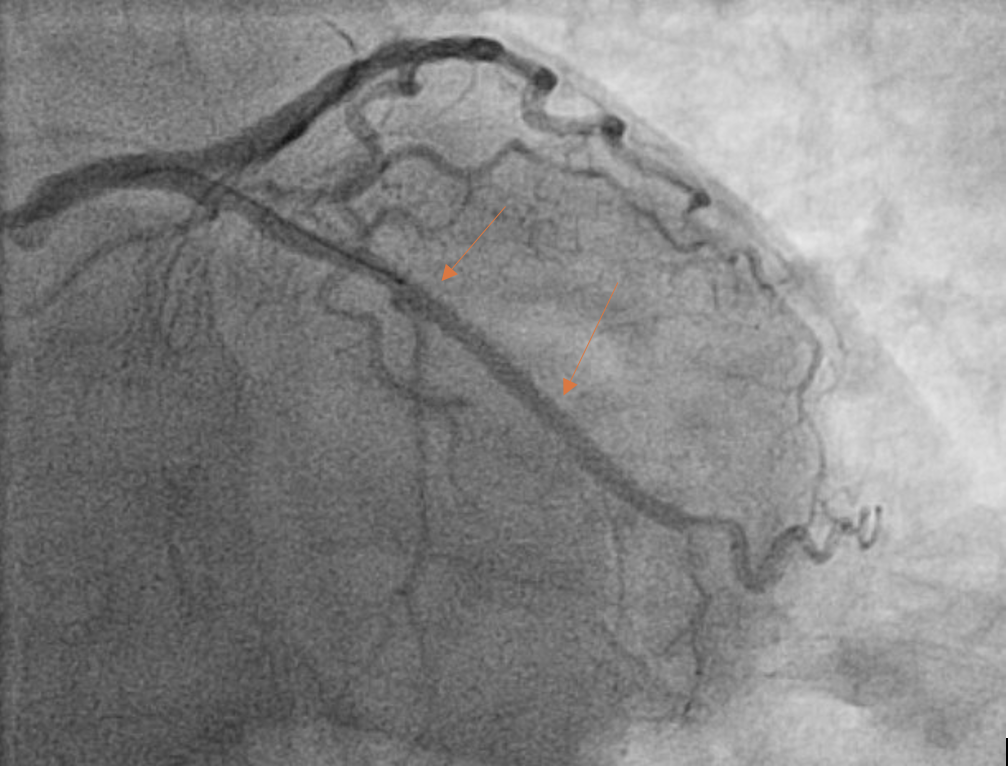
The pre-PCI angiogram reveals complete occlusion of left circumflex (LCx) artery.

The post-PCI angiogram shows successful re-vascularization of LCx.
· Delays in diagnosis, increases the duration of myocardial ischemia and the risk of poor patient outcomes.
· Isolated posterior STEMI (IPSTEMI) cannot be directly diagnosed using standard 12-lead ECG, and often result in missed, or delayed diagnosis.
· Low utilization of 15-lead ECG is postulated to be a causative factor in IPSTEMI diagnostic delays.
· The prevalence and efficacy of 12-lead vs 15-lead ECG on diagnostic delays and clinical outcomes in IPSTEMI in Manitoba has not yet been established.
Why does posterior STEMI show up as ST-depression in V1-V2
· The LCx artery and its obtuse marginal (OM) branches extend to the lateral and posterior areas of the heart.
· In posterior STEMI, LCx arterial occlusion causes tissue ischemia/injury to the posterior heart.
· In STEMI, the electrical “current of injury” travels in the direction from healthy tissue to ischemic tissue.
· Facing electrodes will record these vectors as STE on the ECG.
· The precordial leads V1-V3 record electrical vectors travelling away from these electrodes, as STD.
The importance of 15-lead ECG’s
· Differentiating between anterior endocardial ischemia and posterior epicardial/transmural infarction with a standard 12-lead EKG can be challenging.
· In both instances, STD can be evident in the precordial leads (V1-V2).
· It has been shown that 12-lead ECG fail to identify posterior STEMI, particularly where minimal or absent ST-changes are noted (body habitus, subtle ST-segment changes).
· The posterior leads V8-V9 record electrical vectors travelling toward these electrodes, as STE.
When do we do them? (Manitoba experience)
1. WRHA, St. Boniface Hospital, WFPS, MB EMS
a. Normal 12-lead (CP >15 min)
b. STD V1-V2 with prominent R-waves on 12-lead
c. Acute inferior MI on 12-lead
2. Leads V8, V9, V4R
Manitoba Message
1. Prevalence of isolated posterior STEMI in Manitoba is not known
2. Compliance of 15-lead utilization as per guidelines above is not known
3. Delays in posterior MI recognition and subsequent revascularization occur
a. Clinical outcomes are not known
4. DO THE 15-LEAD!
a. It’s only 3 extra electrodes