
An Interesting ECG Case
Case:
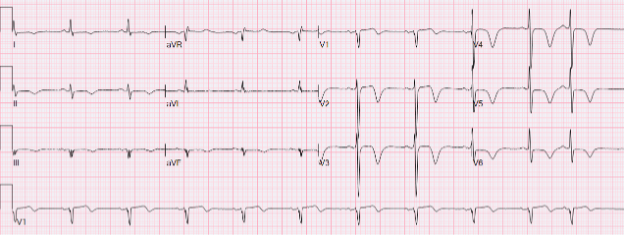
58-year-old man from Thompson with T2DM, HTN, DLD, and current smoking presented with left-sided chest pain and nausea starting Jan 6 @ 02:00. Troponin was elevated and rising (270 → 349 → 482). After presentation, there was no recurrent chest pain. The ECG is shown here:
Is this a STEMI?
No obvious STEMI by classic criteria — there is no clear ST elevation. However, this ECG is high risk: sinus rhythm with marked anterior repolarization abnormality, including deep, symmetric T-wave inversion across the anterior–lateral precordial leads (most prominent V3–V6) with minimal ST-segment shift. In the right clinical context (ischemic symptoms + rising troponin), this should trigger urgent coronary angiography, especially from a remote site.
What is the diagnosis?
This is a classic Wellens ECG pattern — a “warning sign” for a critical LAD lesion and an impending large anterior MI if not managed urgently.
Types of Wellens (quick refresher):
Type A: biphasic T waves, often V2–V3 (≈25%)
Type B: deep, symmetric T-wave inversion in the anterior leads, often V2–V4, sometimes extending to V5–V6 (≈75%)
They can evolve from A → B over hours/days.
This ECG best fits Type B.
Why do the T waves look like this?
A helpful concept: blocked arteries can block and spontaneously unblock. Transient platelet clumping on a ruptured plaque can temporarily stop blood flow, and platelets can also release vasoactive factors that promote local coronary spasm, further reducing flow. When flow partially restores, the ECG can show “reperfusion-type” T-wave changes — while the underlying LAD lesion remains unstable and prone to re-occlusion.
Two takeaways (Manitoba-specific)
1) Remote-site urgency: Wellens = “LAD at risk” even if pain settles
Wellens can look deceptively “stable” (pain resolved, no ST elevation), but it should move the cath plan up the queue. In remote sites, the main hazard is delay — and delayed angiography increases the chance of sudden re-occlusion and a large anterior MI.
2) P2Y12 strategy should match time-to-cath (and CABG risk)
This case also highlights a practical issue:
If angiography can truly occur within 24 hours, it is often reasonable to hold P2Y12 until anatomy is known, because some patients will need CABG.
In this case, he had cath <24 hours, but did require CABG — and because he had already received DAPT, surgery was delayed for antiplatelet washout.
However, many Manitoba NSTEMI transfers from remote sites do not get early cath (delays >36 hours are common). In those situations, where a high risk feature such as Wellens is not present, we still generally recommend DAPT, because the patient is waiting with an ACS and older NSTE-ACS data supports reduced ischemic events with DAPT during the waiting period.
Newsletter pearl: Wellens is an ECG “red flag” for critical LAD disease — and in Manitoba, the key decisions are (1) How fast should we get cath? (2) Should we give P2Y12 now or hold it because cath is truly imminent and CABG is possible?
We will talk about other high risk ACS patients in future Manitoba ACS Network Newsletters.