
An Interesting ECG Case
63F referred for urgent coronary angio due to ongoing chest pain.
•PMHx:
Hypertension
Dyslipidemia
Fibromyalgia
Anxiety
•Presented to the ER at a peripheral hospital with shortness of breath
•Treated as pneumonia
•Developed chest pain that was refractory to analgesics and anti-anginals limited by low blood pressure.
•Cath lab contacted as ongoing chest pain
•Troponin 203 (7:52 AM) -> 603 (10:15 AM)
ECG:
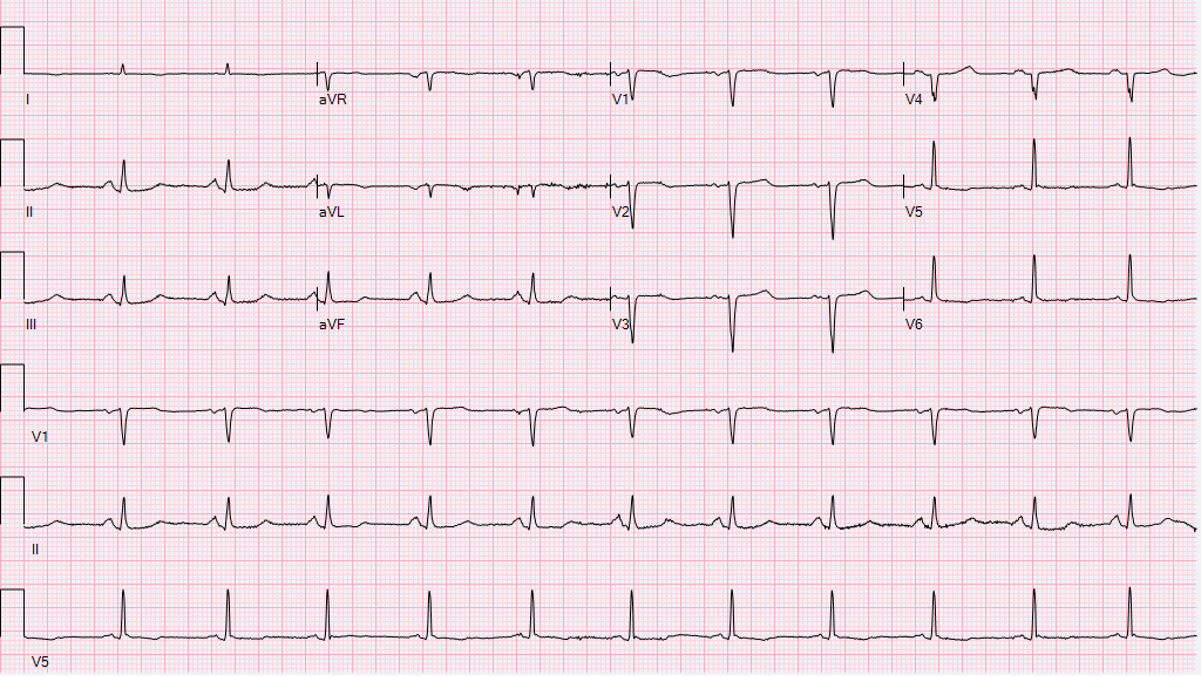
•ECG: sinus rhythm (70 bm), suspicious for anterior infarct, nonspecific ST-T wave changes (lateral T wave inversion/flattening)
Coronary angio:
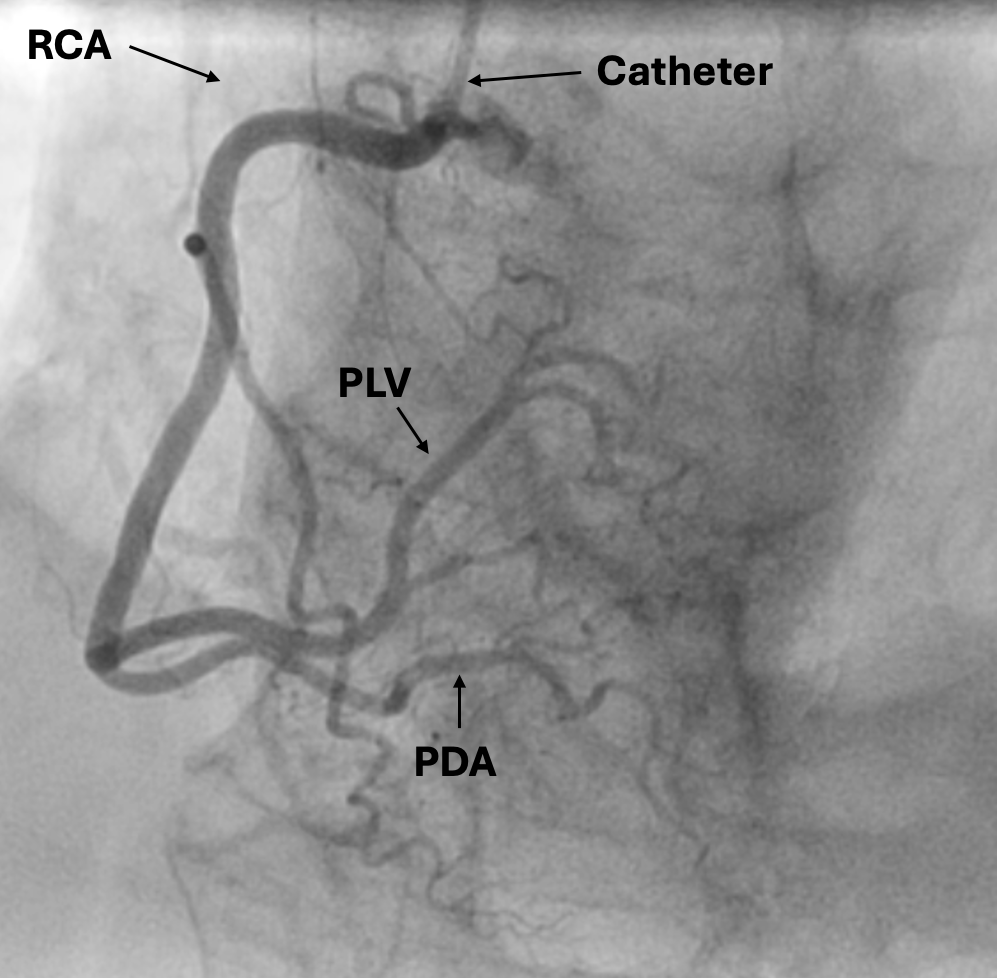
RCA: right coronary artery
PLV: posterior left ventricular artery
PDA: posterior descending artery
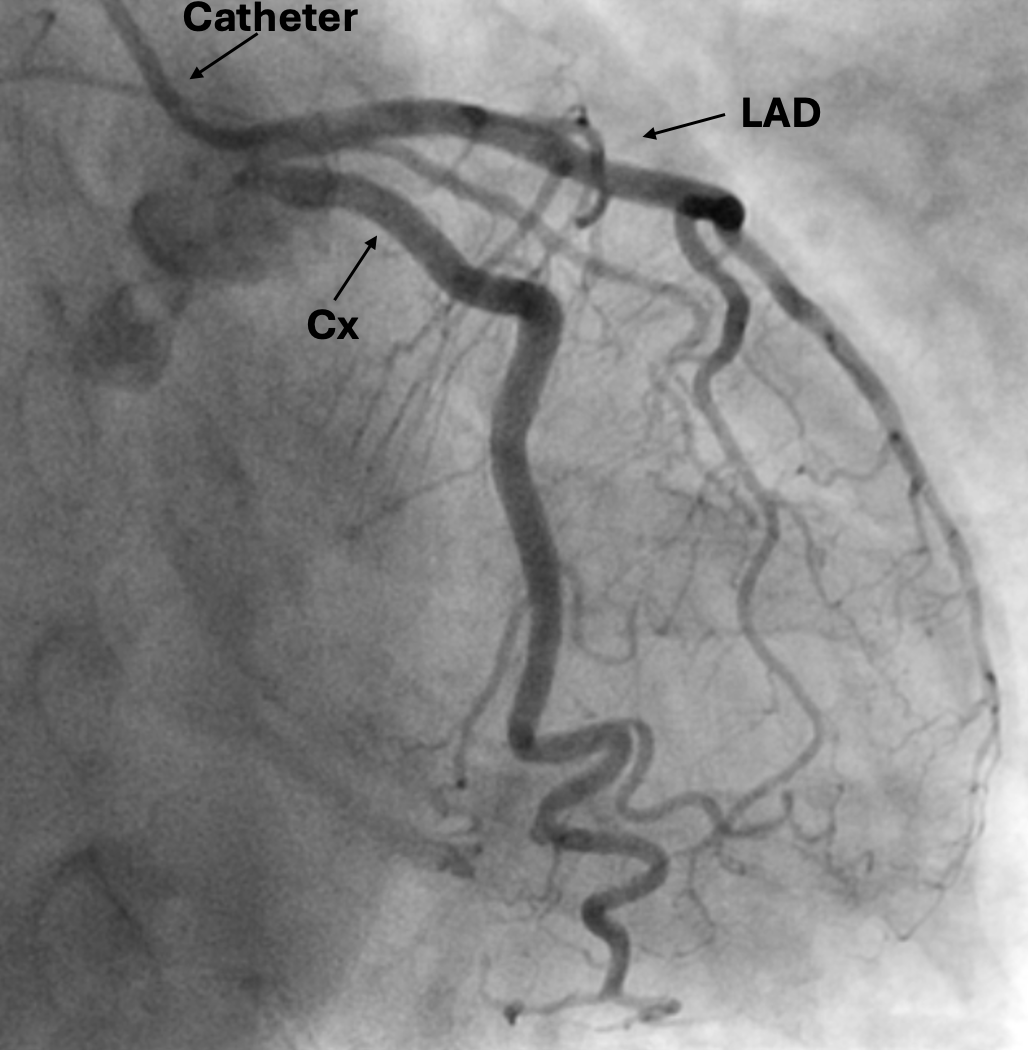
LAD: left anterior descending artery
Cx: circumflex artery
LVgram in diastole:

LVgram in systole:
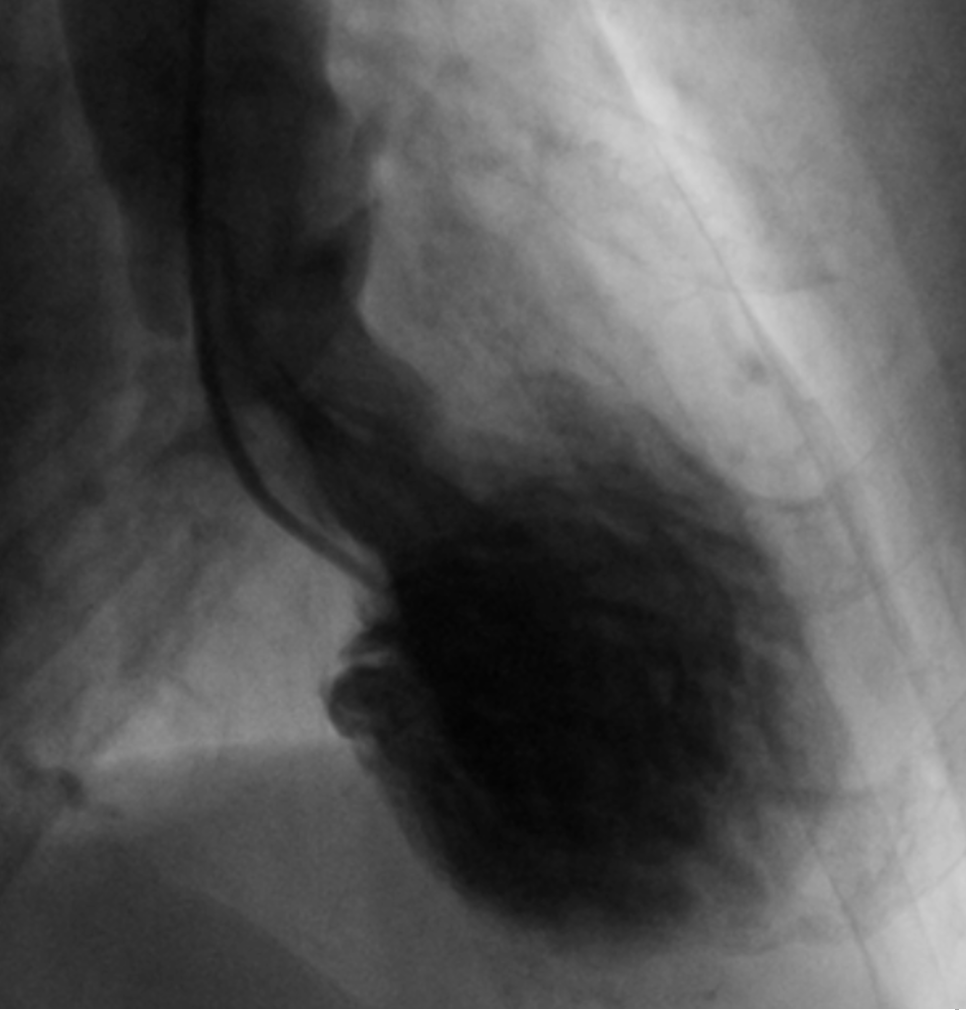
Takotsubo cardiomyopathy
•AKA stress-induced cardiomyopathy, broken heart syndrome
•Transient regional global systolic dysfunction of the left ventricle
•Mimics ACS – can present with chest pain/shortness of breath, troponin elevation and ECG changes
•1-2% of ACS cases
•Often associated with an acute stressor (physical, emotional or mental)
•Often need a coronary angiography to assess for LAD territory ischemia as these can co-exist
•If patient has ongoing CP or STEMI or hemodynamic instability, they may need urgent coronary angio
•Management is usually supportive and guided by the patient’s clinical presentation and hemodynamic status
•Besides medical stabilization, patients may benefit from beta blockers and ACE inhibitors
•If patient’s LVEF is reduced, TTE to reassess LV function in a few months is recommended
Do you want to learn more about Takotsubo cardiomyopathy?
Following along - we will be highlight Takotsubo cardiomyopathy in the next issue!