
An Interesting ECG Case
An 85-year-old male with mild cognitive impairment, permanent atrial fibrillation, CABG 25 years ago and permanent pacemaker for high grade AV block called 911 because of worsening chest pain on the background of his chronic chest pain. No shortness of breath, diaphoresis, or nausea associated with these episodes.
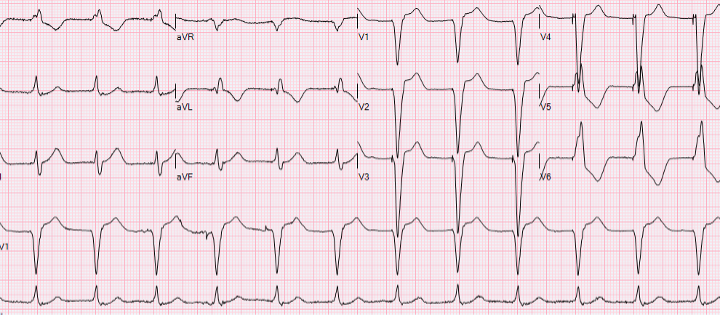
He was found by EMS to by hypotensive (BP 90/60) with the following ECG:

1. What does this ECG show?
· regular wide complex tachycardia at 170 BPM.
· right axis deviation.
· atypical left bundle branch block pattern.
· no findings of AV dissociation on the ECG (no P waves unrelated to QRS complexes, no fusion beats).
· Most likely rhythm is ventricular tachycardia
2. Is he having a STEMI?
This ECG does not show definitive signs of an acute STEMI. While the wide complex tachycardia with left bundle branch block pattern and right axis deviation could be due to a STEMI, it is essential to look for clear ST-elevation in specific leads (e.g. Sgarbossa Criteria). These criteria are not fulfilled. However, a STEMI cannot be ruled out entirely, and further investigation with serial ECGs, new LV wall motion abnormality and typical rise and fall of cardiac biomarkers could corroborate a STEMI diagnosis.
3. What should you do?
· Recognize this patient is not stable.
· Obtain intravenous access and monitor the patient closely.
· Administer oxygen, maintain hemodynamic stability, possibly with fluid resuscitation or vasopressors if hypotension persists
· Given the wide complex tachycardia, ongoing chest pain and moderate hypotension electrical cardioversion must be considered.
· Rapid transfer to the cardiac center for further evaluation, including possible coronary angiography and echocardiography to assess for ischemia or structural heart changes.
Rationale:
The patient's clinical instability, combined with his history of CABG and permanent pacemaker, suggests that immediate stabilization and comprehensive cardiac assessment are crucial. While the etiology of his tachycardia could be multifactorial (e.g., ischemia, ventricular scar, electrolyte imbalance, or pacemaker malfunction), the primary goal should be to address his hemodynamic status and exclude acute coronary syndrome as a cause.
What happened?
The patient was electrically cardioverted. His blood pressure improved to 110/70, and his pain resolved, making ongoing cardiac ischemia less likely
Repeat ECG:
An echocardiogram revealed mild cconcentric left ventricular hypertrophy is present. Ejection Fraction = 50-55%, Inferior akinesia. No significant valve disease. No significant change from previous echocardiogram done 1 year ago
Troponins were drawn twice, 8 hours apart, and did not rise and fall, both values where in mid-200’s. This suggest that a Type 1 myocardial infarction did not occur at time of his presentation.
Diagnosis was ventricular tachycardia from old myocardial scar, no recent STEMI.
Given his age, cognitive impairment and relatively preserved ejection fraction, flat troponin curve, it was decided not to do coronary angiography or implant an ICD. He was started on oral amiodarone and discharged in a few days.