Canadian Cardiovascular Congress: Dr. Shekoofeh Rizi’s Experience
Five things I learned about ACS at CCC2025:
CCC 2025 was a valuable opportunity for me to deepen my understanding of acute coronary syndrome (ACS). Five key insights that stood out were:
• ACS is increasingly recognized as a heterogeneous condition, involving mechanisms such as plaque erosion, SCAD, and microvascular dysfunction, rather than solely plaque rupture.
• Intracoronary imaging (OCT/IVUS) is becoming essential for identifying ACS mechanisms and guiding more precise PCI decisions.
• Balancing ischemic and bleeding risks is now central to modern ACS care, with growing emphasis on individualized antithrombotic strategies and early DAPT de-escalation in high-bleeding-risk patients.
• Persistent sex differences in ACS presentation, particularly delayed and atypical symptoms in women, remain a significant clinical challenge.
• The future of ACS management is shifting toward precision medicine, integrating advanced imaging, biomarkers, AI, and personalized risk stratification to guide targeted treatment.

Dr. Shekoofeh Rizi’s poster:
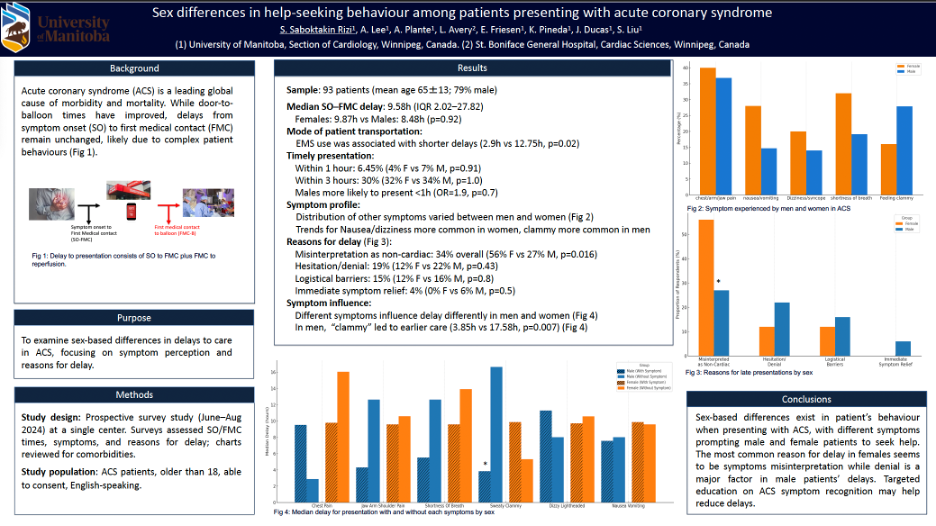
We conducted a prospective single-centre study to understand sex-based differences in help-seeking behaviour among patients presenting with acute coronary syndrome (ACS). Ninety-three patients were analyzed (75.2% male, median age 67±11 years). The median symptom onset-to-first medical contact (SO-FMC) delay was similar between men and women and only 6.5% presenting within one hour. Misinterpretation of symptoms as non-cardiac was the most common reason for delay, particularly among women, followed by hesitation or denial. While feeling sweaty or clammy symptoms significantly shortened delays overall and in males, they were associated with a trend toward longer delays in females. Despite comparable symptom experiences, prolonged pre-hospital delays persisted, underscoring the need for targeted educational strategies to improve symptom recognition and reduce delays, particularly among women presenting with atypical ACS features.
Andrew Lee’s poster:
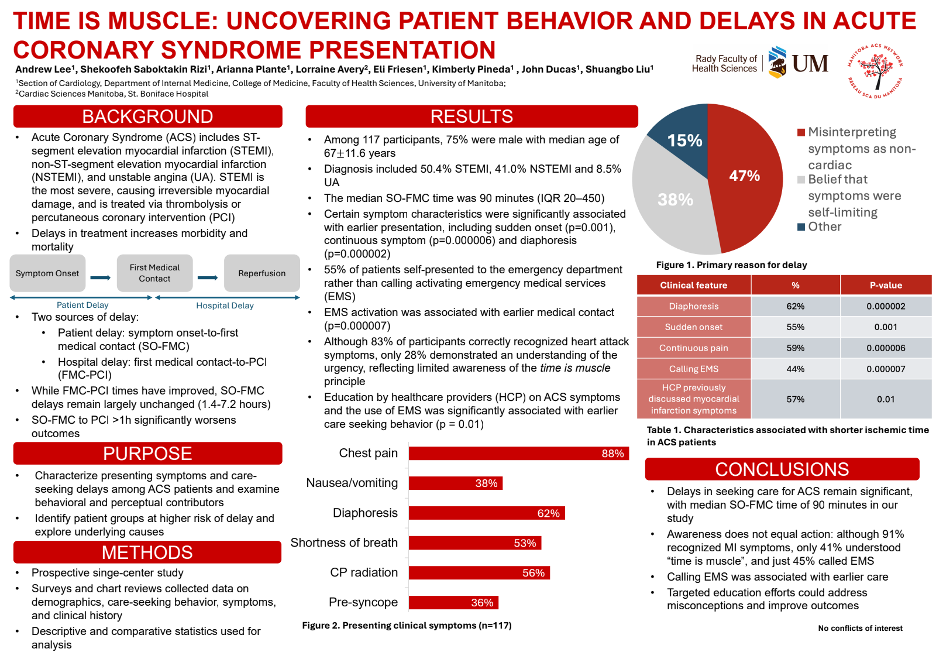
Acute coronary syndrome (ACS) remains the leading cause of death in Canada, and despite improvements in FMC-to-PCI times, delays from symptom onset to first medical contact persist. In this single-centre prospective study of 117 ACS patients (75.2% male, median age 67±11 years), the median SO-FMC delay was 90 minutes, most commonly due to misinterpretation of symptoms as non-cardiac and the belief that symptoms would resolve spontaneously. Chest discomfort, diaphoresis, and shortness of breath were the most frequent symptoms, with sudden onset, continuous symptoms, and diaphoresis associated with earlier presentation. EMS activation was linked to earlier presentation. Although most patients were aware of heart attack symptoms, fewer recognized the urgency of timely care. These findings highlight key targets for focused public education to reduce delays and improve ACS outcomes.