
An Interesting ECG Case
34 year old male presents with chest pain
• No past medical history and not on any medications
• Felt unwell 15 minutes ago while playing basketball
• Having chest pain, palpitations and presyncope
• At triage: HR 235, BP 99/70
• Taken straight to resus
ECG:
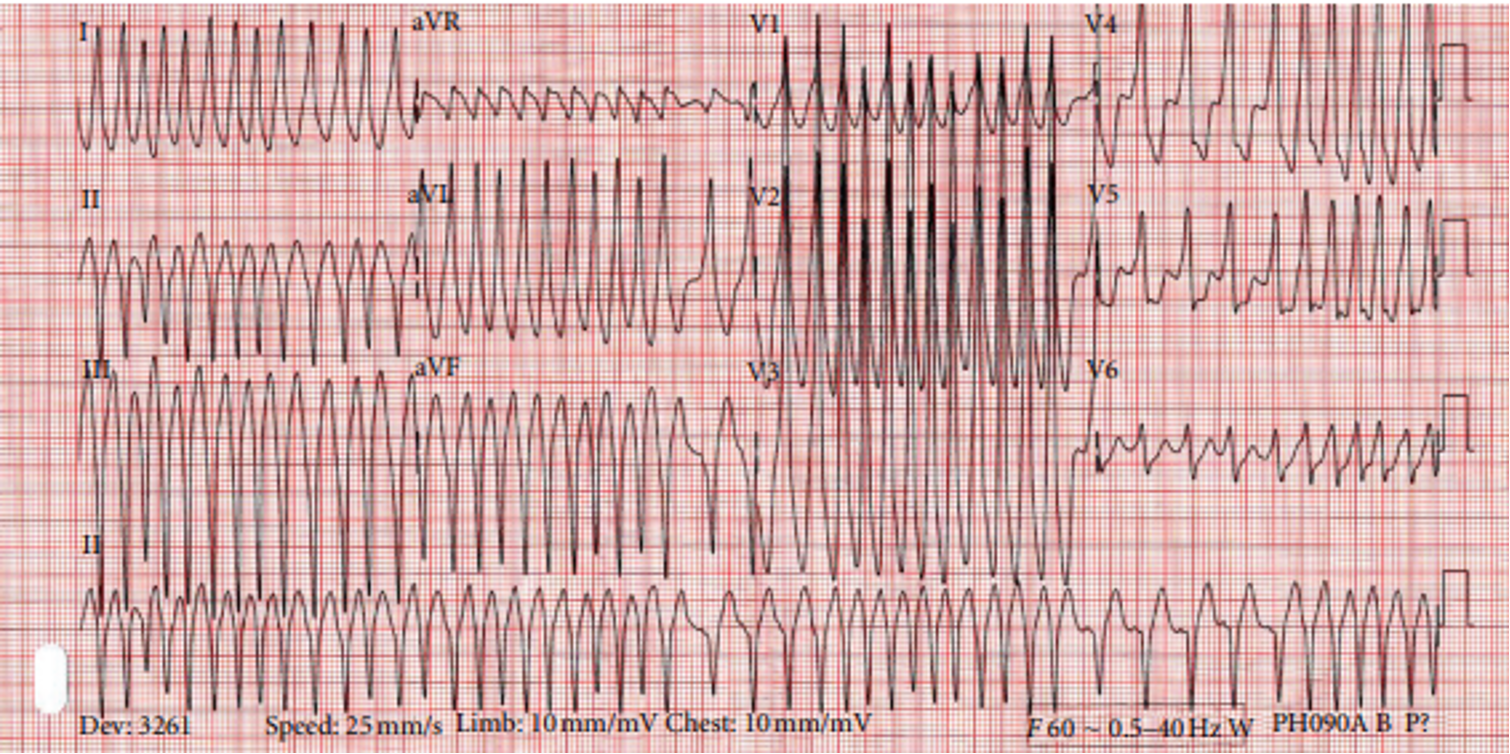
Explanation
• This is atrial fibrillation with preexcitation pattern (Wolff Parkinson White)
• The irregularly irregular rhythm is suggestive of atrial fibrillation rather than a very rapid monomorphic ventricular tachycardia
• The ventricular rate is very fast as the presence of an accessory pathway allows for rapid conduction to the ventricles by bypassing the AV node
• The QRS’s are wide and variable because preexcitation can produce slurred, bizarre ventricular activation because conduction occurs outside of the normal conduction pathway
Treatment
• Unstable patient: synchronized DC cardioversion
• Stable patient: procainamide (Class I antiarrhythmic that slows conduction through the accessory pathway and prolongs the action potential without AV node blocking effect)
• Refer to EP for accessory pathway ablation
• Avoid AV nodal blocking agents (adenosine, beta-blockers, calcium channel blockers, digoxin) as they may preferentially block conduction through the AV node and promote conduction down the accessory pathway, potentially leading to extremely rapid ventricular rates and degeneration into ventricular fibrillation